Qunibi W, Hootkins R, McDowell L, Meyer M, Simon M, Garza R et al. Treatment of hyperphosphatemia in hemodialysis patients: The Calcium Acetate Renagel Evaluation (CARE Study). Kidney Int. ; 2004; 66:s33-38
Treatment of hyperphosphatemia in hemodialysis patients: The Calcium Acetate Renagel Evaluation (CARE Study)
Background
Hyperphosphatemia may cause hyperparathyroidism, osteodystropy and calcification. It has been associated with mortality in observational analyses in hemodialysis patients. More intense methods to control serum phosphate are necessary.
This is an American study and in the United States the most commonly prescribed phosphate binder is calcium acetate. Sevelamer hydrochloride was recently introduced on the market at the time this trial was released.
Trial Design
This was an 8-week, randomized, double blinded, placebo controlled trial.
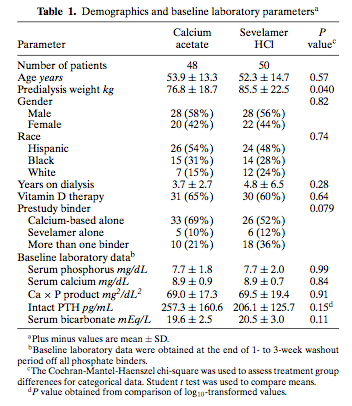
Population
Ninety-eight hemodialysis patients from two study centers: University of Texas Health Sciences Center and the Austin Diagnostic Clinic. Patients were on hemodialysis for at least 3 months, receiving a stable dose of phosphate binder and IV vitamin D.
**The study demographics are shown in a chart below.
Intervention/Comparator
Patients who had a serum phosphorus > 1.93 mmol/L after a washout phase from their original binder were randomized to receive either calcum acetate or sevelamer HCl.
Primary and Secondary Outcomes
Efficacy of calcium acetate and sevelamer hydrochloride to lower serum phosphorous <1.78 mmol/L (< 5.5 mg/dL).
Results
Over the 8-week timeframe, calcium acetate recipients had lower serum phosphorus (1.08 mg/dL difference, P = 0.0006), but higher serum calcium (0.63 mg/dL difference, P < 0.0001). Eight of the forty-eight patients in the calcium acetate arm experienced hypercalcemia.
Limitations
This study was short in duration, had a small sample population and external validity is questionable. It is common practice to use calcium carbonate (calcium acetate was used in the trial) and to take phosphate binders with meals (drug was administered half before meal and half after meal).
Bottom Line
Calcium acetate controls serum phosphorus more effectively than sevelamer hydrochloride.
Treatment of hyperphosphatemia in hemodialysis patients: The Calcium Acetate Renagel Evaluation (CARE Study)
Background
Hyperphosphatemia may cause hyperparathyroidism, osteodystropy and calcification. It has been associated with mortality in observational analyses in hemodialysis patients. More intense methods to control serum phosphate are necessary.
This is an American study and in the United States the most commonly prescribed phosphate binder is calcium acetate. Sevelamer hydrochloride was recently introduced on the market at the time this trial was released.
Trial Design
This was an 8-week, randomized, double blinded, placebo controlled trial.
Population
Ninety-eight hemodialysis patients from two study centers: University of Texas Health Sciences Center and the Austin Diagnostic Clinic. Patients were on hemodialysis for at least 3 months, receiving a stable dose of phosphate binder and IV vitamin D.
**The study demographics are shown in a chart below.
Intervention/Comparator
Patients who had a serum phosphorus > 1.93 mmol/L after a washout phase from their original binder were randomized to receive either calcum acetate or sevelamer HCl.
Primary and Secondary Outcomes
Efficacy of calcium acetate and sevelamer hydrochloride to lower serum phosphorous <1.78 mmol/L (< 5.5 mg/dL).
Results
Over the 8-week timeframe, calcium acetate recipients had lower serum phosphorus (1.08 mg/dL difference, P = 0.0006), but higher serum calcium (0.63 mg/dL difference, P < 0.0001). Eight of the forty-eight patients in the calcium acetate arm experienced hypercalcemia.
Limitations
This study was short in duration, had a small sample population and external validity is questionable. It is common practice to use calcium carbonate (calcium acetate was used in the trial) and to take phosphate binders with meals (drug was administered half before meal and half after meal).
Bottom Line
Calcium acetate controls serum phosphorus more effectively than sevelamer hydrochloride.